

Decisions at all levels of health care need to be informed by reliable high quality data in order to ensure good outcomes and equitable care.

Approach
We are gathering global and local evidence on health information system interventions and characterizing the role of paper-based systems in three LMIC countries. Then, in creative partnership with those countries, we plan to engage in co-creative, collaborative and intentional design activities to redesign the tools and processes to improve paper-based systems. We will then use robust experimental study methods to test the effects of paper-based design interventions on the quality and use of data and on health systems outcomes. We will share the knowledge and lessons learned over the course of the project with decision and policy makers in the global health community.
Workstreams
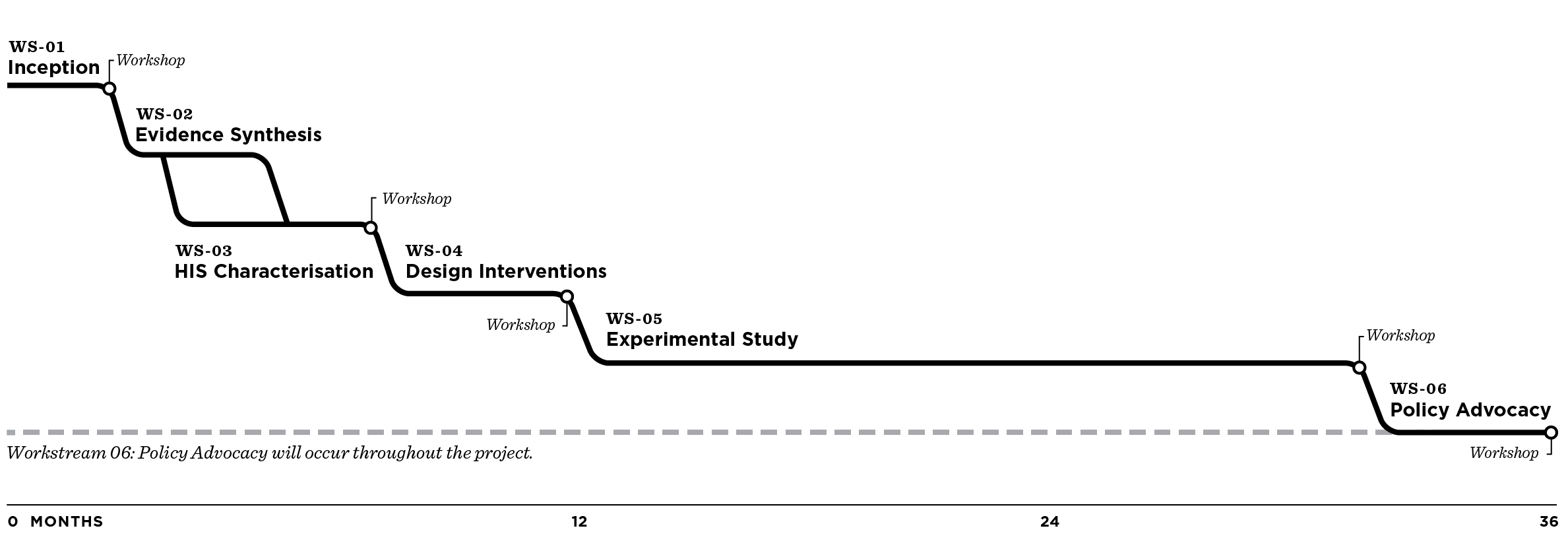
Workstream 1
Inception
During this workstream, we will set up the technical protocols for the other work streams, solidify commitments to engage with each partner country at policy and managerial levels, and establish contractual arrangements with all stakeholders, including country partners and “policy shapers.”
One page overview (WS1) / Approximate duration: 6 months
Workstream 2
Evidence Synthesis
The aim of this workstream is to synthesize all available evidence on interventions to improve HIS. Special attention will be given to the specific barriers interventions are meant to address, effects on reported outcomes and implementation and contextual issues. This synthesis will be carried out using literature systematic review methods and will guide both the qualitative, design research plan and the subsequent design of tailored interventions to be tested in countries.
One page overview (WS2) / Approximate duration: 6 months
Workstream 3
Characterization of HIS
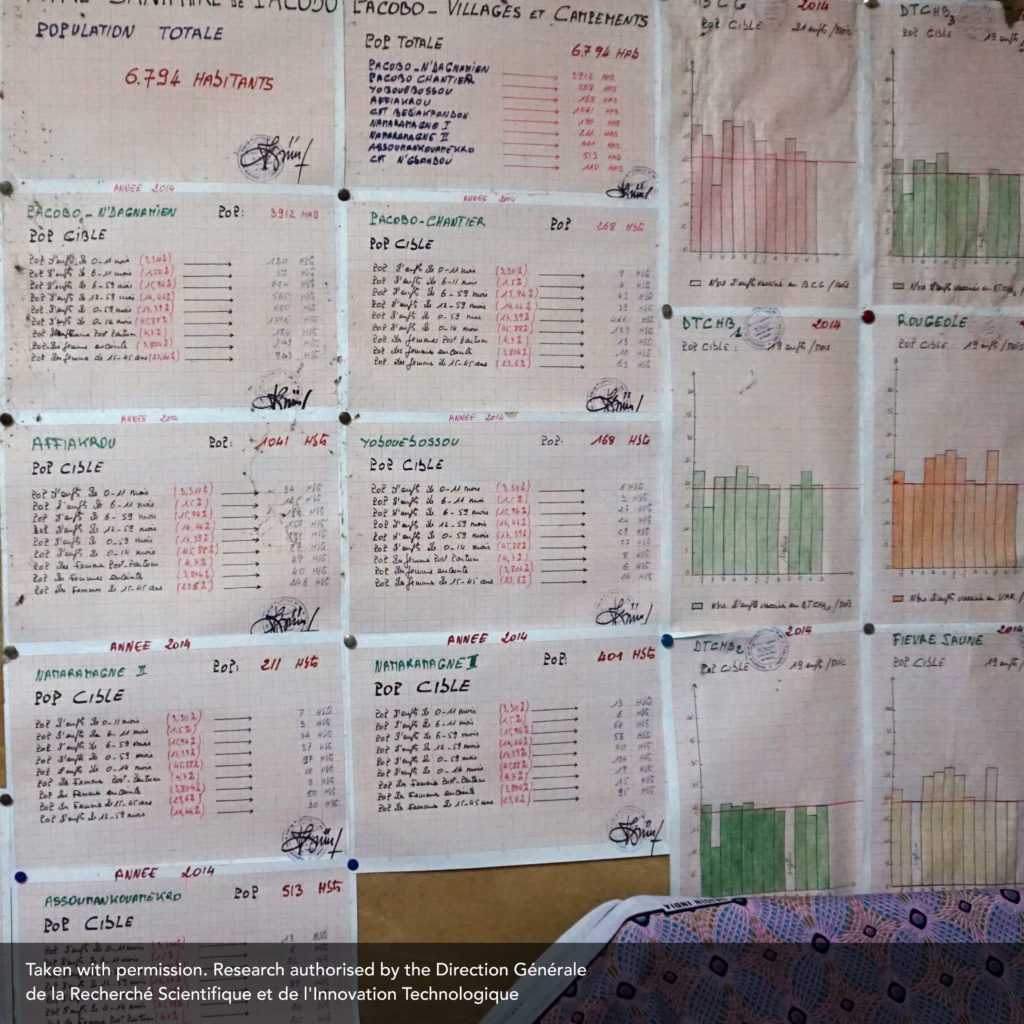
In partnership with our in-country research teams, we will use qualitative and mixed methods to map the current design of the HIS and the experiences of those who use them. To help us identify the strengths and weaknesses of the current systems we will interview, observe, and shadow health workers and beneficiaries who produce and use the data. Our research will identify opportunities for redesigning tools, forms and processes.
One page overview (WS3) / Approximate duration: 3 months
Characterisation of the Health Information Systems in Nigeria, Côte d’Ivoire and Mozambique
Côte d’Ivoire (Exec Summary – French)
Mozambique (Exec Summary – Portuguese)
Nigeria (Exec Summary – English)
Full reports (English only): Côte d’Ivoire, Mozambique, Nigeria
Workstream 4
Design of Paper-Based Interventions
Design thinking does not make strict, sequential divisions between research analysis and design. Our design interventions will be created in a series of iterative dialogues with in-country health workers, government officials and members of the local design community. The extent and content of these designs will emerge out of the identified opportunity areas and will include tools, platforms and process designs as well as the design of change management and training activities. The evidence to support these activities will come from WS2 and WS3.
One page overview (WS4) / Approximate duration: 3 months
Workstream 5
Experimental Studies
Interventions designed in WS4 will be tested in countries using robust experimental study designs aiming at assessing their effects on selected outcomes. Workshops will be held in each country in order to agree on designs, to validate the findings and to discuss their implications for policy and practice.
One page overview (WS5) / Approximate duration: 20 months
Workstream 6
Policy Advocacy & Engagement
From the start of the project, efforts will be made to facilitate collaborative engagement with stakeholders in each country, including primary care health workers, government officials and ‘policy shapers’. Towards the end of the project, final recommendations and technical white papers will be packaged in user-friendly formats targeting several audiences, including national officials, decision makers, and the international research community. A final dissemination workshop will take place in order to explain the findings and advocate for their use.
One page overview (WS6) / Approximate duration: 4 months